if you would like to support my site hosting fees and help keep Haembase #FOAMed forever you can do so here!
Thrombotic thrombcytopenic purpura (TTP) (bsh 2023, BSH 2012)

Intro
MAHA - MicroAngiopathic Haemolytic Anaemia - red cell fragmentation + thrombocytopenia
TMA - Thrombotic MicroAngiopathy - MAHA + pathological features of occlusive micro/macrovascular disease
TTP - Thrombotic Thrombocytopenic Purpura - One type of TMA, caused by ADAMTS13 deficiency
Incidence of acute idiopathic TTP: 0.8 per million of pop. (3.6 per million new hospital admissions) in UK
Untreated mortality: >90%
TTP Pathophysiology
Acquired (auto-antibodies, iTTP) or Congenital (cTTP) deficiency of ADAMTS13
ADAMTS13 – a metalloproteinase responsible for cleaving ultra large VWF multimers (ULVWF)
In the absence of ADAMTS13, ULWVF causes spontaneous platelet aggregation under conditions of high shear stress, e.g. microvasculature, brain, heart, kidneys.
Thrombocytopenia results from consumption within platelet-rich thrombi
Anaemia results from mechanical fragmentation of red cells through partly occluded vessels.
TTP Clinical Features
TTP is a diagnosis suspected from clinical features, then later confirmed by laboratory assays.
Defined as MAHA with mod-severe thrombocytopenia and associated organ dysfunction.
Presenting Clinical Features:
Thrombocytopenia (epistaxis, bruising, petechiae etc)
Central neurological (confusion, headache, paresis, seizures, apahasia, dysarthria, visual disturbance, encephalopathy, coma
Fever >37.5oC
Jaundice (unconjugated hyperbilirubinaemia)
Renal impariment (proteinuria, microhaematuria)
Cardiac (chest pain, heart failure, hypotension, cardiac arrest)
GI Tract (abdominal pain, pancreatitis, ischaemia)
Non-specific (pallor, jaundice, fatigue, arthralgia, myalgia)
Note:
33% No Neurological Signs
Fever and renal impairment may not be prominent
TTP Ix
FBC: Median plt count 10-30 & Hb 80-100 at diagnosis
Film: thrombocytopenia, schistocytes/fragments
Haemolysis markers: Low haptoglobins, Raised Retic, Raised LDH, Normal DAT
Coag screen: Normal
Trop T : Raised in 50%, poor prognostic sign
Others: B12/Folate/Iron
ADAMTS13 Assays
<10% +/- presence of an inhibitor confirms the diagnosis
TTP vs HUS – A level of <5% has 90% specificity for TTP
Activity, Antigen and Autoantibody assays available.
Activity assays based on the failure of patient plasma to degrade VWF multimers
Ix to exclude other causes of MAHA/TMA
Pregnancy Test
Infection: HIV, Hep A/B/C, Stool culture for E.coli
AutoImmune: TFT, Glucose, Autoantibody screen
Cardiac: ECG, Echo
Neuro: CT/MRI Brain
Malignancy: CT CAP, tumour markers
Differential Diagnosis of MAHA/TMA
Acquired TTP
Congenital TTP
Biallelic recessive variants in ADAMTS13 gene. Presents at any age. Often asymptomatic until a precipitating event sends a chronically low ADAMTS13 even lower.
Disseminated Intravascular Coagulation (DIC)
Pregnancy
HELLP, Eclampsia, AFLP
Diagnostically difficult. Pregnancy may be precipitant for 5-25% of TTP cases
Haemolytic Uraemic Syndrome (HUS)
E. coli shiga toxins
Atypical HUS (aHUS)
Excess activation of alternate complement pathway
May be genetic, acquired autoantibody or idiopathic
Drugs
15% of MAHA cases
TTP - Quinine, tacrolimus, simvastatin, interferon, OCP, trimethoprim
HUS – Gemcitabine, bleomycin, mitomycin-C
Malignant Hypertension
Malignancy
Adenocarcinoma especially. Early or late stage disease. ADAMTS13 not low.
Post-HSCT
Lack of ADAMTS13 deficiency, poor response to PLEX. Anecdotal use of defibrotide
Infection
CMV, Adenovirus, Herpes Simplex, Hep B, Hep C, Meningococcus, Pneumococcus, Fungal
HIV – may be presenting feature. ADAMTS13 <5% associated with a relatively higher CD4 count
Autoimmune
Autoimmune Haemolysis, Lupus nephritis, Scleroderma, Evans Syndrome, Vasculitis
Pancreatitis
Malignant hyperthermia / heat shock
Severe aortic stenosis / paravalvular leaks
Catastrophic Antiphospholipid Syndrome (CAPS)
diagnostic scoring systems
Scores may aid identification of TMA patients who are most likely to have TTP. However, they have not been prospectively validated and sensitivity/specificty may decrease with patient age.
Treatment of Acute TTP
1. Start Plasma Exchange (PLEX) within 4-8 hours of suspected diagnosis
Removes offending antibody and VWF Multimers
Replaces ADAMTS13
Delivery:
1.5x plasma volume exchange daily for 3 days, then re-assess
Continue PLEX until plt count >150 (Complete remission), then stop (provided on caplacizumab)
Use SD-FFP to reduce risk of TTI & adverse immune responses.
(Note: MB-FFP associated with longer hospital stay and greater number of exchanges)
(Rock et al NEJM 1991 for PLEX vs Plasma transfusion survival)
2. Caplacizumab
First dose should be given IV pre-plasma exchange (but do not delay PLEX for this)
See next section for details
3. Start steroids
Stop production of antibody
1g IV Methylprednisolone or 1mg/kg PO Prednisolone
Dose and length of treatment varies between centres
Expect an exacerbation of symptoms+thrombocytopenia 7-10 days after steroids
4. Rituximab (Off license)
Stop production of antibody
Dosed every 3-4 days
Reduces No. of PLEX, length of stay and time to CR
Median 10 days to effect —> better outcomes if given early
Some centres give to all patients, some only to those with cardiac/neuro complications
Prolongs time to relapse but no difference in overall relapse rate vs no ritux (Doyle 2023)
5. Supportive Care
Avoid platelet transfusion
PPI
Folic Acid
Prophylactic LMWH once plt count >50 (SD-FFP deficient in protein S)
(Avoid aspirin until caplacizumab complete)
Red cell transfusion if required
Consider Hep B vaccination
6. Follow-up
Life-long term follow-up to manage physical and psychological effects of treatment and monitor for relapse
Screen for memory, neurological, cardiac and renal impairment
Assess for anxiety/depression
7. Difficult scenarios
In cases refractory to standard treatments a wide range of immunosuppressive / immunomodulatory therapies have been used, including:
MMF, Ciclosporin, Azathioprine, Daratunumab, Bortezomib, Vincristine, Cyclophosphamide
Splenectomy
caplacizumab
Pharmacology
28kD bivalent camelid Nanobody, targeting A1 region of VWF
(Camelid’s produce heavy-chain only antibodies which are stable and fully functional)
Theory: release platelets from their ULVWF-bound state, returning them to the circulation
Benefits
Reduces duration of thrombocytopenia, exacerbations, refractory disease, admission duration, PEX procedures and volume of plasma used.
It does not address the underlying disease.
Side Effects
Reduced VWF activity —> bleeding. Severe bleeding rare but VWF concentrates can be considered.
Dosing
First dose should be given IV pre-plasma exchange (but do not delay PLEX for this)
10mg SC after 1st exchange then 10mg daily SC for 30 days
If ADAMTS13 <10% at day 30 —> continue to 60 days
Is Plasma Exchange still needed? (2022)
JTH 2020 case series demonstrated success of TTP treated with caplacizumab without plasma exchange. Updated data presented at ISTH 2022.
Phase 3 trial now open (as of 2023)
TITAN Study NEJM 2016, Phase II
30 days capla for TTP diagnosed based on clinical basis (ie pre-ADAMTS13 level result)
Could not recruit, stopped early, ?Poor study design (Drug have to be given before PLEX)
Despite this, did show reduced time to platelet recovery, reduced exacerbation, but higher relapse
Conclusion: Bridging therapy that reduces microthrombi but does not treat the underlying disease
HERCULES NEJM 2019, Phase III
Randomised, double-blind, placebo-controlled, multi-national study
Plasma exchange allowed prior to starting drug
Able to extend drug beyond 30 days if ADAMTS13 level still low, or if exacerbation occurs.
Reduces No. of exchanges, volume of plasma, No. of ICU days, No. of days in hospital
SE: More bleeding, but minor sites and severity (nose, gums) – theory: organs don’t bleed as full of microthrombi, skin and epithelium has the space to bleed. Aim to manage symptoms, but do not stop caplacizumab.
Further Details of Plasma Exchange
£3,000 per exchange (including cost of SD-FFP)
Two methods of separation - Centrifugal or Filtration
Removes ultra large vWF, replaces ADAMTS13 and removes inhibitor (e.g. antibody)
FFP contains around 1 unit ADAMTS13 per 1ml/kg. So 15ml/kg --> Raise ADAMTS13 by up to 15% (however rapidly consumed or deactivated by antibody)
Replace 1-1.5x plasma volume & takes 110-150 minutes per exchange
Flow rate around 120ml/min through machine
Centrifuge at 2400 rpm
ACD-A anticoagulant
Perform daily until platelet count >150 on 3 consecutive days, then wean off.
Specific Scenarios
Relapse
Defined as an episode of acute TTP occurring >30 days after remission
Can be averted by ADAMTS13 monitoring and pre-emptive rituximab
Relapse rate: 30% at 3 years
40% pts w/ ADAMTS13 relapse have symptoms b4 onset of clinical TTP - usually headache/lethargy
Frequency of relapse does not affect response rate to Rituximab
Congenital TTP (syn. Upshaw-Schulman Syndrome)
Consider long-term prophylaxis – SD-FFP transfusion every 10-20 days
Alternative: ‘8Y’ - a intermediate purity FVIII concentrate containing ADAMTS13
Recombinant ADAMTS13 available on compassionate access schemes (2022), phase 3 trial in progress, expected to replace FFP / 8Y in the future.
Supplement during pregnancy
Pregnancy-Associated TTP
cTTP and iTTP can both present for first time in pregnancy. >40% risk of fetal loss
DDx: HELLP, Eclampsia, aHUS
Treate with PEX and steroids. Caplacizumab not currently recommended in pregnancy. Small molecule, expected to be able to cross placenta.
Fetal thrombocytopenia is not expected
Monitor levels for rest of current pregnancy and throughout future pregnancies
HIV-associated TTP
Wide range of causes for TMA in HIV
True TTP in HIV responds to PEX, steroids, caplacizumab and HAART
————————————————-
lab notes on adamts13 assays
ADAMTS13 Indirect Activity ELISA
Technozym is one supplier. Takes 4-6 hours.
A microtitre plate is coated with anti-GST, subsequently bound to VWF73.
A source of ADAMTS-13 is then added (Calibrator, Control or Patient).
Cleavage of the substrate allows HRP antibody to bind to the remaining fragment --> colour change

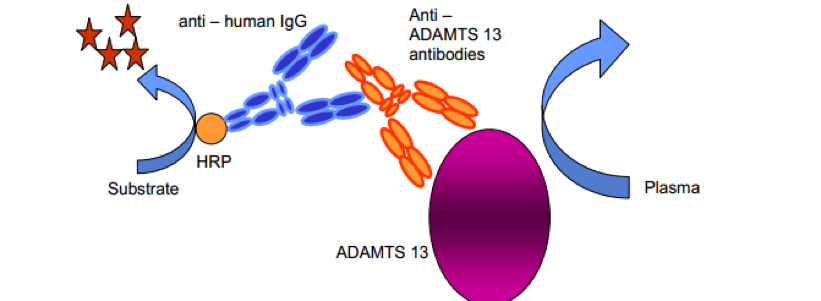
ADAMTS-13 Inhibitor ELISA
To distinguish acquired from congenital TTP
Technozym is one supplier
A microtire plate is coated with recombinant ADAMTS-13.
When incubated with a source of ADAMTS-13 inhibitor (Claibrator, Control, Patient), the antibody will bind to ADAMTS-13.
Addition of an HRP antibody will produce a colour change
(Simple alternative: 50:50 mix with normal plasma)
Other ADAMTS-13 Assays
Antigen
may be normal in TTP, uninformative without activity assay
Direct Activity
SDS Gel Electrophoresis – incubate vWF with plasma and measure the drop in multimer size compared to diluted normal plasmas. Complicated and time consuming.
SDS PAGE & Western blotting – similar to above
FRET Assays – fluorescent resonance energy transfer
Anti-ADAMTS13 Autoantibodies
50/50 mix with normal plasma